
Fittingly, the technology that once sank German U-boats during World War II is now giving middle-aged men erections — including me.
Shockwaves were first discovered in 1939, when the British Royal Navy dropped depth charges to attack German submarines. They rarely exploded close enough to sink them, but shockwave pulses from the blast forced the submarines to the surface, where naval gunfire could finish them off. Despite no shrapnel in the water, the body interprets the pulses as injurious and generates the healing processes neovascularization and neurogenesis (i.e., the creation of new blood vessels and nerves) to deal with that feeling. Eighty years later, the same phenomenon (albeit a low-intensity version) has been proven to have an 80 percent success rate at treating vascular-related erectile dysfunction.
There’s actually a long history of acoustic shockwave therapy — not to be confused with the more controversial electroshock therapy in which seizures in the brain are electrically induced to treat “mental disorders,” including women and gay men in the past — being used therapeutically. It was first employed in 1980 to break up kidney stones in an intense procedure called lithotripsy, during which the patient was sedated and placed in a tub of lukewarm water where pulse waves targeted the stones. Twenty-five years later, European scientists demonstrated the efficacy of treating coronary artery disease in a similar manner.
In 2009, Israeli urologist Yoram Vardi figured that if shockwave therapy worked in the small vessels of the heart, it might also work in the penis as well, since most men with ED have vascular problems (poor blood flow is ED’s leading cause). To prove his theory, Vardi tested a low-intensity shockwave on 20 men with mild or moderate ED twice a week for six weeks. Erectile function improved significantly in 15 of the men, 12 of whom no longer needed Viagra or the like. While such drugs are extremely effective at treating ED, Vardi argued, they provide only functional improvement without treating the root case. Shockwave therapy, he suggested, could be a game changer.
In the procedure, low-level shockwaves are directed at various locations on and around the penis, including the left and rights sides of the groin, where the pudendal nerve meets this pelvis; the corpus spongiosum, where the penis dives behind the testicles (aka the taint); and along major blood vessels and nerves on the shaft. The pulse waves bust up micro plaques, or calcification on the inside of very small blood vessels in the penis. That said, urologist Judson Brandeis cautions me that no one can prove this as doing so would require shockwaving a 70-year-old man’s dick before cutting it off to look at it under a microscope. But we have learned from rats that shockwaves boost the number of new blood vessels in the penis, leading to stronger erections.
While I’ve never really suffered from ED, like the balance of my 42-year-old doughy frame, my boners aren’t as rigid as they once were, which is how my feet land in the stirrups of Dr. Cheryl Geer, one of 356 MDs in the U.S. offering GAINSwave treatment for ED. It’s not a device per se; rather, it’s the brand name for a set of protocols created in 2017 by Mark White and Richard Gaines, anti-aging doctors in Florida.
My knees wobble slightly as I ascend the stairs to Geer’s second-floor office in an outdoor shopping mall abutting a manmade lake in Westlake Village, California. Like most GAINSwave providers, Geer offers a package of six shockwave treatments for $3,000 and a dozen for $5,500, which aren’t covered by insurance. “I like value,” she explains while we sip La Croix and chat in a well-appointed waiting room before the procedure. “Most places only give 5,000 pulses; I give almost three times that, but still use GAINSwave prices.”
An OB-GYN, Geer was introduced to GAINSwave after treating her female patients with vaginal lasers. Those with breast cancer couldn’t have sex due to anti-estrogen hormones causing their vaginas to become atrophic. “Their rainforest becomes a desert, turning plums into prunes,” she says. She was thrilled that the lasers offered a non-hormonal treatment that worked for them, but due to prolonged periods without sex, their husbands had developed ED. “If you don’t use it, you lose it, and husbands stopped functioning. I thought, There has to be a solution to this.”
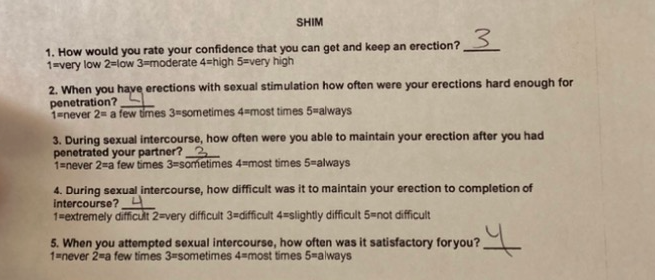
Snacking on carrots and chocolate-covered almonds in Geer’s waiting room, I’m directed to complete the Sexual Health Inventory for Men (SHIM) test to measure my erectile function. On a scale from 1 to 5, I’m prompted to consider:
- How confidently I can get an erection
- Whether it’s hard enough for penetration
- How often I can maintain it following penetration
- My overall satisfaction with sexual intercourse.
I score an 18, which puts me in the “mild ED” category (22-25 means no ED; 17-21 is mild; 12-16 is mild to moderate; 8-11 is moderate; and 5-7 is severe).
“We’re trying to build a bonfire, so everything we do is either fuel or cold water,” Geer explains delicately. She cites alcohol and tobacco as examples of the latter, and plant-based Mediterranean diets with healthy fats and high-quality animal proteins as examples of the former. The same goes for the Priapus Shot (aka “P-Shot”), which processes blood with platelet-rich plasma before injecting it back into the penis. Geer recommends a P-Shot in conjunction with the GAINSwave treatment to supercharge the process. In addition to the number of pulses administered, another variable of the treatment is the kind of device used. Geer initially had one from a company in Hong Kong but she didn’t think it was high-quality enough, so she bought a $40,000 system made by German medical company Zimmer.

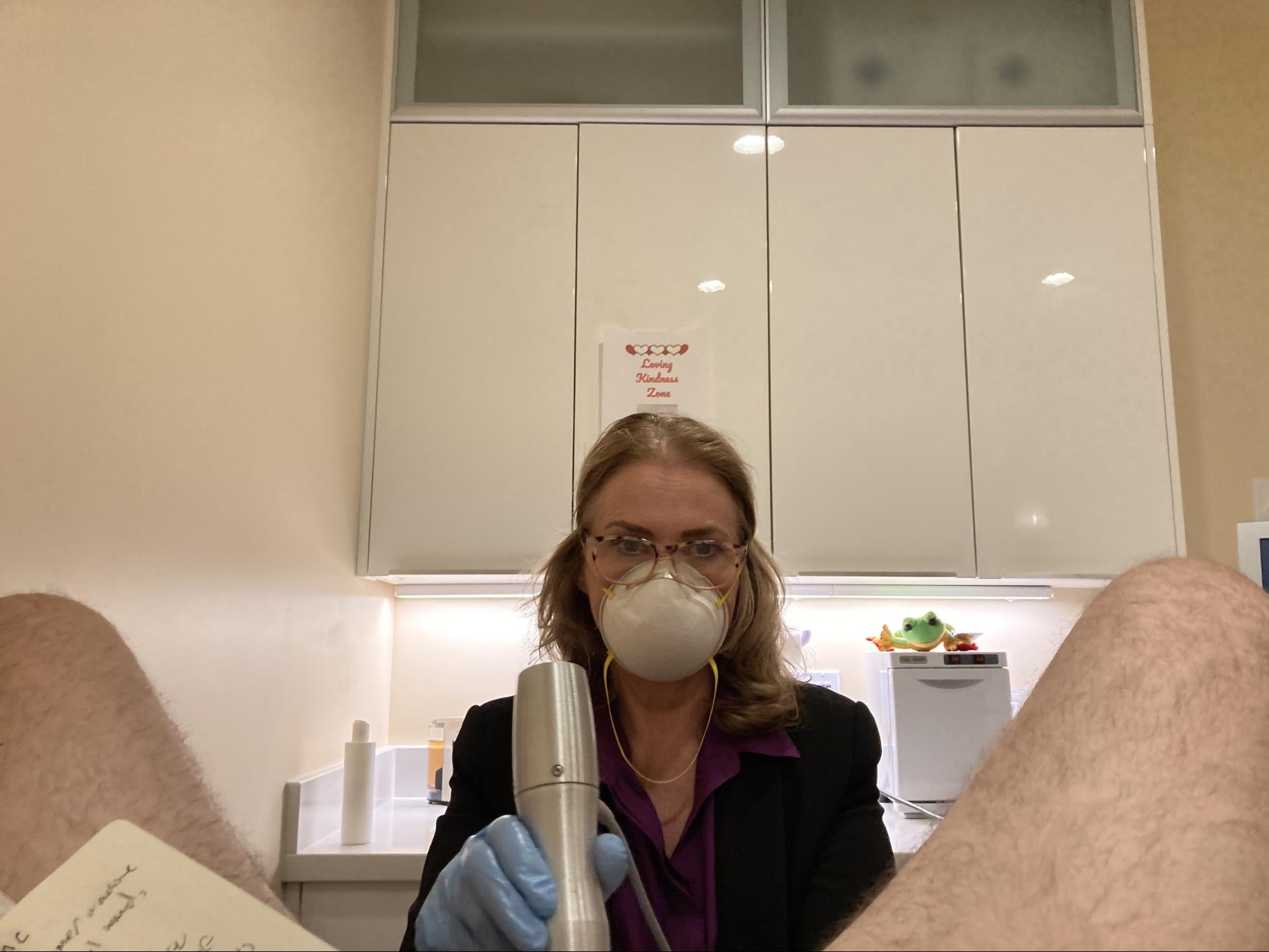
Passing a wand-like device attached to the Zimmer, Geer directs me to disrobe from the waist down and sit on a doctor’s table under a blanket with both legs in stirrups before excusing herself. An instrumental version of Eric Clapton’s “Tears in Heaven” plays as I peer up at Botticelli’s “Birth of Venus” painted on the ceiling. “I wanted something cool on the ceiling so people on the table would have something to look at,” she tells me when she returns.
Unholstering the Zimmer, Geer explains that she will be administering 14,000 pulses to the pudendal area, the left and right lateral penis (3 and 9 o’clock on the shaft), the corpus spongiosum and the head. “Give me your hand,” she says, raising what looks like a giant silver dildo. “I’m going to show you what it feels and sounds like.”
Given that it sounds like a jackhammer, I’m tentative about the feel part of that equation, but thankfully, it’s essentially just a noisy massager. After applying oil to avoid chafing, we begin with 4,000 pulses on both sides of my taint where the pudendal nerve enters the pelvis and spiders out like a Christmas tree to feed the entire genital area. “Good,” she says over the loud THWAP THWAP THWAP of the Zimmer. “I can see every blood vessel and tributary on the shaft of your penis, which I’m treating as well. No pain, right?”
Mercifully, no. People have the wrong idea about shockwave therapy and think it’s electrocution, Geer says, assuring me that there are no jumper cables in the office. “It’s an acoustic shock.” And while GAINSwave protocol calls for numbing cream, Geer doesn’t use it. One of her patients, a porn star, said the numbing cream made it feel like he left his penis in the glove compartment. “Also, you can’t use your penis for hours after it’s been numbed, so adult entertainment performers could really hurt themselves. That’s where Peyronie’s comes from: bad aim. Then there’s scar tissue, then a bend.”
While an impressive number of men with ED find benefits with shockwave therapy, many others do not. As Paul Nelson, a men’s sex therapist at Maze Men’s Health in NYC, tells me, it only treats erectile dysfunction caused by poor blood flow. “That’s not always the case for every situation with ED,” he explains. “Sometimes ED is from poor blood-trapping mechanisms, sometimes it’s from poor nerve function, everyone is different.”
In terms of my own blood flow, I glance down and mortifyingly realize my penis is swelling, the thick dorsal vein noticeably pulsing. “Sorry about that,” I sigh, sinking into the table, completely embarrassed.
Luckily, my burgeoning erection doesn’t faze Geer one bit. “You have good circulation!” she commends, graciously explaining that the procedure is meant to cause blood flow to the penis and that erections are common. “It works better with an erection because blood flow opens up the vessels so I can really get in there to blast the plaque off. You just have to be comfortable with it, and confident that I’m gonna move away before it blows. That I’ve never had that happen.”
“People want to make this out to be something salacious or vulgar, but it’s not. It’s sacred and precious,” she continues.
Before leaving — the entire procedure only takes about 30 minutes — she orders some bloodwork to test my vitamin D, a bottle of which she hands me to inhibit wound healing. I’ll need it after undergoing significant microtrauma in my penis, she explains.
Did it work in the end?
As mentioned, studies have shown that four out of five men with blood-vessel-related ED have benefited from the treatment, and a 2010 study found all 20 of its participants had experienced improved erectile function after six months of shockwave treatment (admittedly, this is a very small sample size, and I should also mention that the FDA has yet to approve the therapy as a treatment for ED).
Personally speaking, while I haven’t had penetrative sex since the procedure, I did wake myself up twice the night of my appointment after rolling over on my boner, which had never happened before. It’s now a regular occurrence, too, which is nicer than not.
If anything, I like to think of it as my own nocturnal depth charge.

C. Brian Smith
C. Brian Smith writes hard-hitting gonzo features for MEL, whether it be training with a masturbation coach, receiving psycho corporal treatment from a spank therapist, or embarking on a week-long pleasure cruise with 75 Santa Clauses following their busy season.