
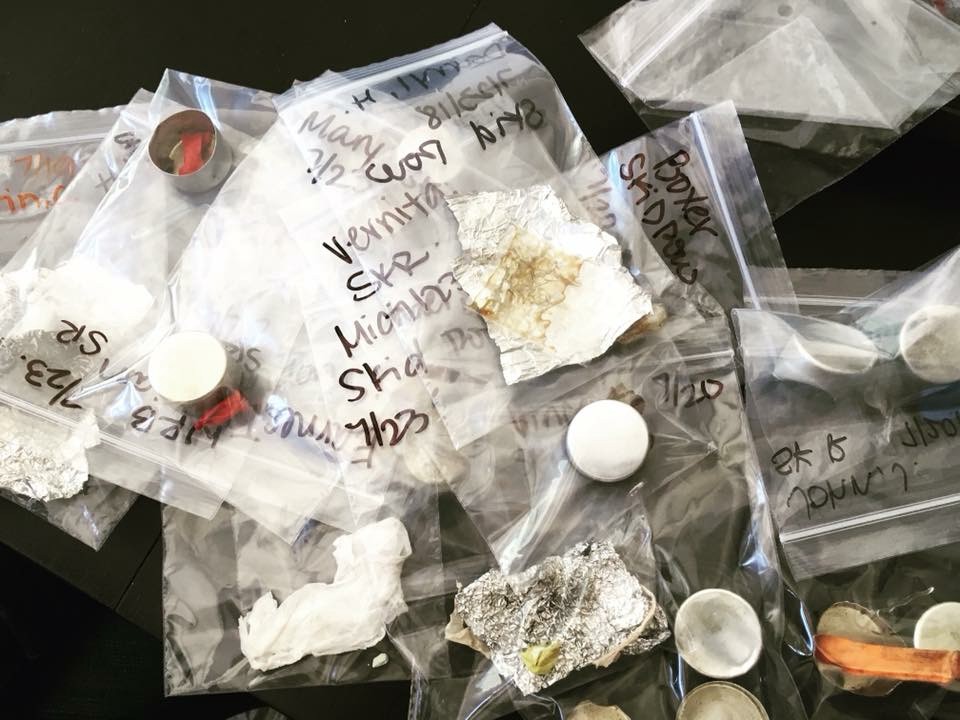
Twenty-year-old Kirsten keeps two hypodermic needles loaded with naloxone, the chemical antagonist used to counter opioid overdoses, in an empty Don Julio tequila box with a red cross scribbled on the side. “The medical bin” as she calls it — brimming with Band-Aids, vitamins and alcohol prep pads — sits just inside the front flap of a burgundy tent she’s pitched near the Egyptian Theater in Hollywood with fiancé Michael, a 37-year-old skateboarder who looks more like her brother than her boyfriend.
After singer Demi Lovato’s apparent overdose last month, her friends reportedly revived her with Narcan, the pricey brand name nasal inhalant version of naloxone that reverses heroin overdoses as well as those from other opioids like fentanyl, morphine and oxycodone. Last month, the Surgeon General encouraged everyone to carry Narcan, now available in all but four states without a prescription, to treat opioid overdoses. (It was the first Surgeon General’s public health advisory since a 2005 warning about prenatal alcohol exposure.) GoodRx lists the price for Narcan at around $135 per package of two applicators — if the first dose doesn’t revive the person, use the second.
When you take opioids — like heroin, morphine or hydrocodone — they bind to, and activate, opioid receptors in the brain, blocking pain, slowing breathing and having an overall calming effect. But when someone overdoses on opioids, they can stop breathing entirely and become unconscious. Naloxone essentially competes with those opioids and kicks them off the opioid receptors. When that happens, the effects of the opioids start to reverse, the person arouses and begins to breathe again.
“I really should’ve gotten stitches two weeks ago,” Michael tells me, pointing to a self-inflicted knife wound on his palm that’s healing surprisingly well. He then grins at his bride-to-be. “Thank God there’s a doctor in the family.” (Or at least someone who attended two months of nursing school before dropping out because she “couldn’t be in Missouri anymore.”) “My grandmother is a nurse,” Michael says. “My Aunt Kelly is a nurse. My mama was a nurse.”
Even though he nor Kristen are addicted to opiates (they’re amphetamine junkies if anything), both of them consider it a sacred duty to save human life should the need arise. “Two of my best friends are dead right now because of this fucking drug,” Michael explains, one of whom OD’d on his daughter’s second birthday — with her sitting on his lap. “I hate heroin with a passion,” he adds. “But I love Naloxone and never go anywhere without it. (Kirsten and Michael’s manually injected vials of naloxone are far less expensive than Narcan; they distribute them for free — as is the case with most needle-exchange programs in the country.)

I meet the engaged homeless couple in a parking lot behind the Los Angeles LGBT Center in Hollywood, where, twice a week, the L.A. Community Health Project (LACHP) operates a mobile needle exchange and naloxone distribution center. When I arrive at 6 p.m. on a recent sweltering Sunday afternoon, I find Program Coordinator Megan Nicolaides arranging dozens of heroin cookers, cotton swabs and tourniquets on a table in front of a large white van. Offering snacks and bottles of water, she warmly greets clients who deposit fistfulls of used needles into secure receptacles in exchange for clean ones — and as much Naloxone as they want.
“If you suspect someone’s overdosed and they’re not responding,” Nicolaides counsels, “give them a strong shake and a ‘sternum rub’ by digging a knuckle into the center of their chest.” (Other addicts suggest face slapping, ripping out chest hair, placing an ice cube in the armpit and/or a swift kick to the nuts.) Next, she says, announce, “I’m going to give you Narcan if you don’t acknowledge me.” (Narcan is like “getting donkey punched with adrenaline,” Michael says, which immediately ruins your high.) If the person can respond by voice he or she will be okay, Nicolaides explains — they needn’t even make sense so long as the response is cued by you.
Clear signs someone needs Narcan, however, include blueing of the lips and fingernails and/or an inability to breathe normally. “Give it to them immediately if you hear anything sounding like respiratory struggle,” she instructs. This may include shallow breath, irregular breath, no breath or what she calls a “death rattle” wheezing sound. There’s no medical consequence to administering Naloxone to someone who’s not overdosing, she adds, so when in doubt, always hit them with it.
To do so, she explains, load one dose of clear liquid into an intramuscular needle and inject the entirety into a muscle, ideally the bicep or upper butt. (Not into the heart, she cautions, despite many believing this to be correct based on Vincent Vega’s harrowing intervention in Pulp Fiction.) If they don’t wake up in a minute, Nicolaides says, give them the second dose and dial 911. “We educate clients about Good Samaritan Laws on the books in all 50 states, which offer legal protection to people who give ‘reasonable assistance to those who are injured, ill or otherwise incapacitated.’”
“That Good Samaritan law is bullshit,” chimes Travis, a homeless addict who arrives to re-up on clean needles and Narcan. After hearing the death rattle of a friend recently, he called 911 and was promptly handcuffed upon police arrival. So now he takes matters into his own hands, stockpiling Naloxone and distributing it as an insurance policy wherever he hangs out.
The natural high of saving a human life doesn’t last long either, Travis says, because the practice is now commonplace thanks to a recent trend of fentanyl-laced heroin flooding the market. “It’s like a Narcan party out there,” he says, adding that he’s personally saved 17 lives with naloxone. His friend Brian puts that number at well over 30. “It’s sadly so normal for us,” Brian explains. “We’re around it all the time. The first and second time, it’s really surreal, and the high does last a day or two. But after the 10th time, the 15th time, the 20th time, it starts to be no big deal.”
“Tolerance change is the number one risk factor for opiate overdose,” explains LACHP Executive Director Michael Marquesen, who tells me most of the clients he lost this year had been in and out of jail or in rehab for months and then tried to use exactly as they did before. When I ask him who, in 2018, should have naloxone on hand, he says way more people than currently do. “People whose kids are using drugs. People whose friends are using drugs. People whose roommates are using drugs. People with homeless drug addicts in front of their apartment building. I’ve trained a cancer patient who’s on serious pain medication who often forgot if she’d taken them. I showed her daughter how to use Narcan and explained, ‘If mom’s ever non-responsive, do this.’”
Travis recently prepared a clean 27-gauge needle — the one he uses to shoot heroin — and filled it the top with Naloxone for “a rich white kid from a good family with a bright future ahead of him” who’d taken a 60-day break from opiates. “As soon as I dumped it, he went from blue and stutter-breathing to normal in a matter of seconds.”
Brian Sullivan was saved by Naloxone, too. He attempted suicide in 2006 by ingesting the entirety of his late mother’s methadone and pain medication only to be revived by paramedics using Narcan. Like the Surgeon General, it’s convinced him that almost everyone should carry Narcan — especially considering the opioid epidemic we find ourselves in. “We’re losing 144 people a day,” he notes. “That’s the equivalent of three jets crashing to the ground a week.” He adds that his home state of Tennessee had 1,631 opioid overdose deaths last year and is the third most prescribed state when it comes to legal prescription opioids. As such, he thinks it’s “foolish” not to keep Naloxone on hand if anyone in your life is at risk of opioid abuse.
On a more callous note, it’s also the fiscally responsible thing to do. The cost of an overdose runs anywhere from about $3,500 to $8,500 depending on the participation of first responders, the cost of an ambulance ride to the hospital, the number and kind of tests for complications (plus HIV and Hepatitis C tests for intravenous drug users) and the length of the subsequent hospital stay. On the flip side, while the price of Naloxone can vary greatly depending on your state, your insurance plan and the type you want to buy, the generic version costs between $20 and $40 per dose. And again, most needle exchanges provide the drugs free of charge.
Obviously, pill pushers and dope fiends are at the greatest risk for opiate overdose, but Marquesen says he’s been getting more and more phone calls, emails and Facebook messages from concerned parents, whom he urges to drop by to stock up on Naloxone. “We train family groups from Orange County because a lot of their kids are using drugs contaminated with fentanyl. People I’ve known since high school hit me up, worried about their kids, siblings or even parents.”
People like Genevieve Przybylo of suburban Chicago. As she told the Washington Post in January, she used Narcan on her 22-year-old son after he’d been on a bender and was taking unusually long showers. When he didn’t respond to her, she forced open the bathroom door to find him “panting, gasping and gurgling.”
“Get the Narcan!” she yelled to her husband.
“I hit my son with it, and he had no reaction whatsoever. His eyes were shut, and he was fading out. I hit him with the second dose, and his eyes opened.” Before long he was awake—if a bit wobbly—and making conversation. Not long after, he voluntarily entered a 90-day inpatient treatment program. If Przybylo hadn’t had the Narcan on hand, she says her son probably would have died. “As a parent, the worst thing is leaning over your child and not being able to help them. Having it available was life-changing.”
And most importantly, life-saving.

C. Brian Smith
C. Brian Smith writes hard-hitting gonzo features for MEL, whether it be training with a masturbation coach, receiving psycho corporal treatment from a spank therapist, or embarking on a week-long pleasure cruise with 75 Santa Clauses following their busy season.