If we’re to believe the myriad online forums on erectile dysfunction, impotence is the greatest curse that can ever beset a man. And the data tell us it’s all too common. Case in point: According to the Cleveland Clinic, as many as 52 percent of men will experience erectile dysfunction in their lifetime, including 40 percent of men age 40 and older and 70 percent of men age 70 and older.
And while those numbers are only slightly higher for men who’ve had prostate cancer — regaining erectile function is basically a 50/50 proposition after a prostatectomy — there is one major difference: The ED they suffer from is more or less permanent. That is, no amount of treatment — whether physical, medicinal or psychological — is going to end their bout of impotence; instead, it’s a lifetime sentence.
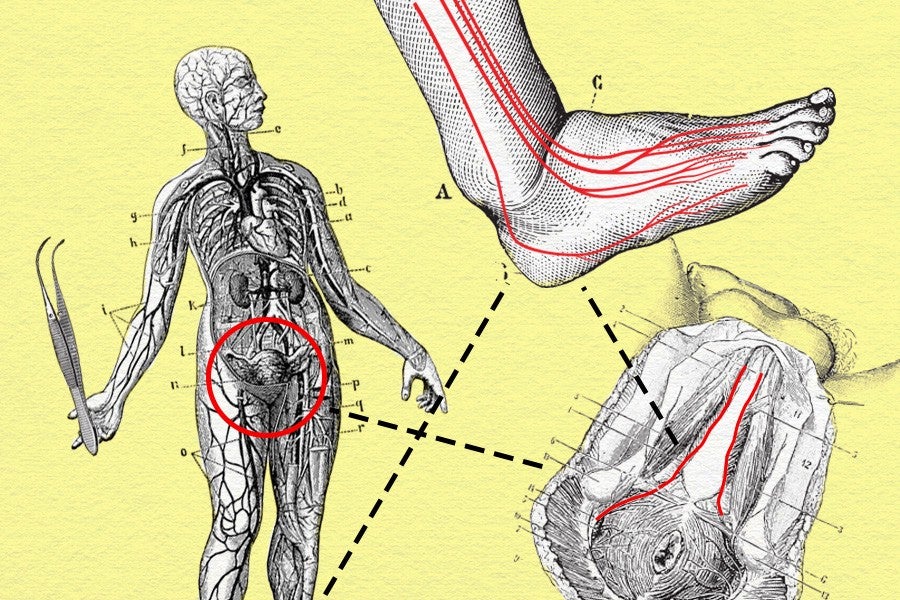
Doctors have spent nearly 40 years attempting to bring some semblance of normalcy to the sex lives of those men who have lost their prostate to cancer. The first breakthrough came in 1981, when Dutch urologist Pieter Donker discovered that the nerves responsible for erections (the cavernous nerves) ran down the sides of the gland, not through it. The discovery got urologic surgeons thinking: Perhaps a prostate could be removed without harming the nerves, thus preserving a man’s erectile function.
Sixteen years later, a surgical team in Texas devised and performed a procedure on a 57-year-old married man during which about 8 inches of his sural nerve (a sensory nerve in the calf) was taken from his foot during the removal of his prostate. Immediately following his prostatectomy, about 3 inches of that nerve was then inserted between the cut ends of each cavernous nerve and stitched into place.
Four months after his surgery, the man began noticing improvement in erectile function. And 14 months later, he was able to have an unassisted erection firm enough for intercourse.
It was a pioneering procedure that Dr. David F. Jarrard, a professor of urology at the University of Wisconsin, has been performing ever since. We recently spoke to Dr. Jarrard to better understand how a nerve from the foot can inspire an erection, the other ways in which cancer can destroy the male member and the chances of surgery being a cure-all for other types of ED.

How many of these grafts have you done personally?
We only do maybe one or two a year. It’s not done frequently because of the strict requirements for a potential candidate. In total, I’ve done maybe 40 or so.
What are the requirements?
The patient has to be young with good expected longevity and good erectile function preoperatively. Furthermore, the cancer has to be a cancer with a higher likelihood of being cured by surgery alone in order to avoid the need for radiation or androgen deprivation therapy [an antihormone therapy whose main use is to treat prostate cancer]. Lastly, the patient has to have undergone a radical prostatectomy in which neither of his cavernous nerves were able to be preserved during surgery. It’s rare that we would perform this procedure on a patient who still has one of his cavernous nerves left intact.
Why does radiation possibly lead to ED?
Radiation may damage nerves in your pelvic area. It also could block blood flow to your penis or decrease the level of testosterone in your body. But in many cases the reason isn’t clear.
Take me through the procedure itself.
A patient will be given general anesthesia so they’ll not be aware of the surgical procedure. After which they’ll also be given antibiotics by injection to help prevent infection. I’ll then make five small incisions in the lower abdomen through which a robotic-controlled camera and other arms will be passed to perform the procedure. I operate a console and manipulate the robot system, which will allow for a clear view of the operation and fine movement controls. I remove the prostate through one of the keyhole incisions and will perform intracorporeal suturing [sewing inside the body] to minimize risks of complications.
After the radical prostatectomy is complete, with the help of a plastic surgeon, I will remove a nonessential nerve from the patient’s leg and reattach it where the nerves surrounding the prostate previously were.
How long is the surgery?
The prostatectomy surgery takes about two hours. The nerve harvesting and grafting adds another 30 to 40 minutes to the procedure since it has to happen concurrently. We’ll harvest the sural nerve while removing the prostate. So it’s just a matter of hooking in the sural nerve where the cavernous nerve that was removed used to be.
Are you eligible to get the nerve graft if you’ve already had your prostate removed?
It has to happen simultaneously since those nerve endings degenerate and retract so you can’t do it in a delayed fashion or after the fact.
What’s the recovery process like?
The graft doesn’t add much recovery time. Most patients, if they have an active job, are back three weeks after the procedure. If it takes, these nerves will grow down the grafts. The grafts are really conduits that provide sheath for nerve growth. Typically, it can taken anywhere from 12 months to 18 months for the nerve endings to regenerate and heal so the patient can begin having erections again.
Are there any side effects?
Some men have experienced discomfort where the nerve was removed from the ankle and numbness on the side of the foot.
Will the erection ever be as strong as it once was?
Some patients function normally, and some require Viagra or Cialis. It depends on the patient and each individual case.
What’s the future of this procedure?
One place we’re moving to is coming up with artificial sheath nerves that serve the same function as a sural nerve. Our hope is to take a manufactured nerve sheath that would save us from having to make any incision in the ankle. This would mean fewer recovery issues. Currently, there are several companies working on this type of artificial sheath that would then be applicable for any sort of nerve-grafting procedure.
Do you ever envision a time in which there would be surgical interventions for ED not related to a prostate issue or prostate surgery?
The development of erectile dysfunction is multifaceted. It can be hormonal, vascular or physiological changes that occur with aging. All of those contribute to problems with erections as someone gets older. This particular procedure is a specific incidence where all that stuff is working well but that section of the nerve has to be removed. That said, because of the emergence of artificial nerve sheaths, it could be possible for this type of surgery to become much more common.
What do you suggest for men who have ED but don’t qualify for this operation?
There are oral medicines like Cialis, Viagra or Levitra. There are other mechanisms as well such as medicines that can be delivered directly to the penis via a pump or vacuum device that traps the blood in the penis. A final treatment option is you can use a penile prosthesis. These devices are either malleable or inflatable. The simplest type of prosthesis consists of a pair of malleable rods that are surgically implanted within the erection chambers of the penis. With this type of implant, the penis is always semi-rigid and merely needs to be lifted or adjusted into the erect position to initiate sex.
One last question about the men whose ED issues are cancer-related: Why is saving their sex life so important?
The goal of any cancer treatment, including surgery, is to cure the cancer and return the patient back to their normal lifestyle. Sexual function is one aspect of this recovery that is critical for many patients.
Andrew Fiouzi
Andrew Fiouzi is a staff writer at MEL.